Portfolio Scoring Guide for UK Specialty Training
How to Maximise Your Audit, Research, Teaching & Presentation Evidence for Oriel, HEE & Foundation Programme Applications
Updated April 2026 · Covers UKFPO, IMT, CST, Radiology, Ophthalmology, Paediatrics & GP Training
Why Building Your Portfolio Early Matters
Whether you are a UK medical student, foundation trainee, or international medical graduate (IMG), the evidence you gather for clinical audit, research, publications, presentations, and teaching directly determines your competitiveness for specialty training posts in the United Kingdom.
Competition for specialty training posts has intensified significantly. For the 2025/26 recruitment cycle, programmes such as Internal Medicine Training (IMT), Core Surgical Training (CST), Clinical Radiology, and Ophthalmology faced competition ratios exceeding 5:1 in many regions. The differentiating factor between shortlisted and unsuccessful candidates is almost always the strength and completeness of their portfolio evidence.
The critical message for medical students is this: do not wait until your Foundation Programme or postgraduate internship to begin gathering this evidence. Many of the highest-scoring portfolio items — completed two-cycle audits, peer-reviewed publications, formal teaching programmes, and conference presentations — require months of lead time. Starting during clinical placements in Years 4 and 5 gives you a significant competitive advantage that compounds throughout your career.
MD ACUMEN supports medical students and early-career doctors in building portfolio evidence that meets the exact terminology and documentation standards required by NHS England (HEE), Oriel, and Qpercom verification panels. Our clinical placements at NHS GP practices provide supervised opportunities to complete closed-loop audits, present findings at multiprofessional meetings, and obtain properly formatted supervisor certificates with GMC verification.
in IMT Self-Assessment
from Portfolio Station
for Maximum Scoring
per Audit Project
Understanding the UK Medical Training Pathway
A structured overview of the training stages and where portfolio evidence becomes critical.
The UK medical training pathway comprises several sequential stages, each with distinct application processes and evidence requirements. Understanding this pathway early allows you to plan strategically and accumulate evidence at each stage.
Medical School (Years 1–5/6)
The ideal time to begin building portfolio evidence. Clinical placements in Years 4–5 provide opportunities for supervised audit projects, research involvement, and teaching experience. Publications achieved at this stage carry forward into every subsequent application. Prizes and additional degrees score highly in several specialties.
Foundation Programme (FY1–FY2)
Since 2024, the UK Foundation Programme uses Preference Informed Allocation (PIA) — a computer-generated random rank — replacing the previous EPM + SJT system. Portfolio evidence no longer counts towards FP allocation. However, everything you achieve in FY1–FY2 carries directly into your specialty training applications. The Specialised Foundation Programme (SFP) offers academic blocks through medical school nomination or PIA.
Core / Specialty Training (CT1/ST1) — Portfolio Evidence Is Critical
Applications to IMT, CST, Clinical Radiology, Ophthalmology, Paediatrics, and other specialties are scored through self-assessment or portfolio stations evaluating audit/QIP, research, publications, presentations, teaching, and leadership. The evidence gathered at medical school and in FY1–FY2 directly determines your shortlisting and interview scores.
Higher Specialty Training (ST3+) & Consultant
Higher specialty applications and the Portfolio Pathway (formerly CESR) for consultant registration require even more extensive evidence. Academic Clinical Fellowships (ACFs) and NIHR Clinical Lectureships require demonstrated research track records including higher degrees (Masters, PhD/MD). A strong portfolio built from medical school provides a continuous evidence base.
Important: IMG Prioritisation from 2026
The Medical Training (Prioritisation) Bill introduces priority access for UK medical graduates to core and higher training places from 2026. IMGs already in the UK who have completed foundation or core training, or who hold ILR, EU settled status, or British dual-citizenship, will also be eligible. A strong portfolio becomes even more important for competitive differentiation. See the BMA guidance.
Portfolio Scoring Domains by Specialty (2026)
How audit, research, publications, presentations, and teaching are scored across major UK training programmes.
| Specialty | Scoring Format | Audit / QIP | Research / Publications | Presentations | Teaching |
|---|---|---|---|---|---|
| IMT | Self-Assessment (30 pts + 5 bonus) |
✅ Points scored | ✅ Points (PubMed 1st author = max) | ✅ Points scored | ✅ Experience + training |
| CST | Portfolio Station at Interview (45%) |
✅ Grade A–E | ✅ Grade A–E (PubMed/DOI) | ✅ Grade A–E | ✅ Grade A–E |
| Clinical Radiology | Portfolio Review (40% of total) |
✅ Academic domain | ✅ Academic (imaging focus) | ✅ Academic domain | ✅ Teaching & Training |
| Ophthalmology | Self-Assessment (max 47 pts) |
✅ Points scored | ✅ Points scored | ✅ Points scored | ✅ Points scored |
| Paediatrics | Application Form (30 pts / assessor) |
✅ QI Projects | ✅ Academic Achievements | ✅ Academic domain | ✅ Transferable Capabilities |
| GP Training | MSRA Only (no portfolio) |
❌ Not scored | ❌ Not scored | ❌ Not scored | ❌ Not scored |
| Foundation (UKFPO) | PIA Allocation (no portfolio) |
❌ Not scored | ❌ Not scored | ❌ Not scored | ❌ Not scored |
Key insight: While GPST and the Foundation Programme no longer score portfolio evidence, all other major specialty training programmes do — and the evidence you gather during medical school and foundation training carries forward. Building your portfolio early is an investment that pays dividends across multiple application cycles.
Clinical Audit & Quality Improvement Projects (QIP)
The single most important portfolio domain for the majority of UK specialty training applications.
Audit and QI evidence is scored in virtually every specialty that uses portfolio assessment. The hierarchy is consistent: a completed two-cycle (closed-loop) audit where you led all aspects and demonstrated measurable change scores maximum points. A single-cycle audit scores mid-range, and basic data collection participation scores minimum.
The HEE Seven-Stage Audit Cycle
NHS England (formerly HEE) recognises seven stages in a completed audit cycle. For maximum scoring, you must provide evidence of completion at every stage.
| Stage | Required Activity | Evidence Tip |
|---|---|---|
| 1. PLANNING | Define audit criteria and clinical standard (e.g. NICE guideline) | Document the standard in your audit report title and introduction |
| 2. DATA COLLECTION | Collect baseline data (Cycle 1) | Record methodology, sample size, data sources (e.g. EMIS search) |
| 3. DATA ANALYSIS | Analyse Cycle 1 results against the standard | Include tables/charts showing gap between performance and standard |
| 4. IMPLEMENTING CHANGE | Design and deliver interventions to address gaps | Document specific interventions (recall systems, education, coding changes) |
| 5. SECOND CYCLE (Closing the Loop) |
Re-audit after intervention; compare to Cycle 1 baseline | This is the critical step — without it you cannot score maximum points |
| 6. DEMONSTRATED CHANGE | Show measurable improvement in outcomes | Quantify the change (e.g. "17 additional patients vaccinated") |
| 7. REFLECTION & SUSTAINABILITY | Reflect on findings; establish ongoing monitoring | Document lessons learned and sustainability plan in your report |
Audit Scoring Hierarchy (Typical Across Specialties)
| Score Level | Description (HEE / Oriel Terminology) | Typical Score |
|---|---|---|
| Maximum (Option A) |
Lead in ALL aspects of a QI project or audit which demonstrated change through a completed second cycle / closed audit loop. Participated in all stages: planning, data collection, data analysis, implementing change, and involvement in both cycles. | 6 pts (IMT) Grade A (CST) |
| High (Option B) |
Lead in all aspects of a QI project or audit which demonstrated change (single cycle with measurable improvement) | 4–5 pts Grade B |
| Mid (Option C) |
Contributed to multiple cycles of a QI project or audit which has demonstrated change | 3 pts Grade C |
| Low (Option D) |
Participated in data collection for a project led by someone else | 1–2 pts Grade D |
| None (Option E) |
No evidence of audit or QI involvement | 0 pts Grade E |
Strategy for medical students: Choose audits with high patient turnover, clear NICE guideline standards, simple and achievable interventions, and the ability to re-audit within your placement period. A 4–6 month clinical placement is typically sufficient to complete both cycles of a focused QI audit using PDSA methodology.
Required Evidence Documents for Each Audit Project
Three documents form the complete evidence package that satisfies HEE/Oriel verification requirements.
When you upload your audit evidence to Oriel or Qpercom, verifying clinicians will check that your documentation matches your claimed score. If the evidence does not match, your score will be downgraded. The three required documents are:
1. Signed Supervisor Letter (Audit Certificate)
A formal letter from your named clinical supervisor confirming your role and level of involvement. Must include: the supervisor's full name, designation, and GMC number; a statement confirming you were "Lead in ALL aspects"; confirmation that the project "demonstrated change through a completed second cycle / closed audit loop"; confirmation of participation in all stages: planning, data collection, data analysis, implementing change, and involvement in both cycles; and the supervisor's signature and date.
2. Meeting Confirmation Letter (Presentation Evidence)
A separate letter confirming you formally presented the audit findings at a recognised meeting. Must include: the project title; the presenting author(s) with you named as first author; the date of presentation; the meeting name and venue; the meeting organiser's name and role; a description of the content presented; and the organiser's signature with GMC number.
3. Presentation Slides (PowerPoint / PDF)
A copy of your actual presentation with your name as first author on the title slide. Should demonstrate: both cycles of data; the intervention/change strategy; results showing measurable improvement; and reflective analysis. The presentation should be clearly attributed to you and your co-authors.
Qpercom Upload Requirements
Evidence is uploaded to Qpercom (the digital evidence verification platform used by NHS England). Only images (max 5MB) or PDF files (max 10MB) are accepted. File names must not contain special characters (&, £, %). Once you click "Finish and Submit," no further edits are possible and recruitment administrators cannot upload on your behalf. See NHS England Qpercom guidance.
Example Certificate Templates
Redacted examples of the audit certificate and meeting confirmation letter that meet HEE/Oriel requirements.
The following redacted templates illustrate the format and content required for a supervisor letter (audit certificate) and a meeting confirmation letter. These use the exact HEE terminology expected by Oriel self-assessment panels and Qpercom verification reviewers. All personal details have been redacted for illustration purposes.
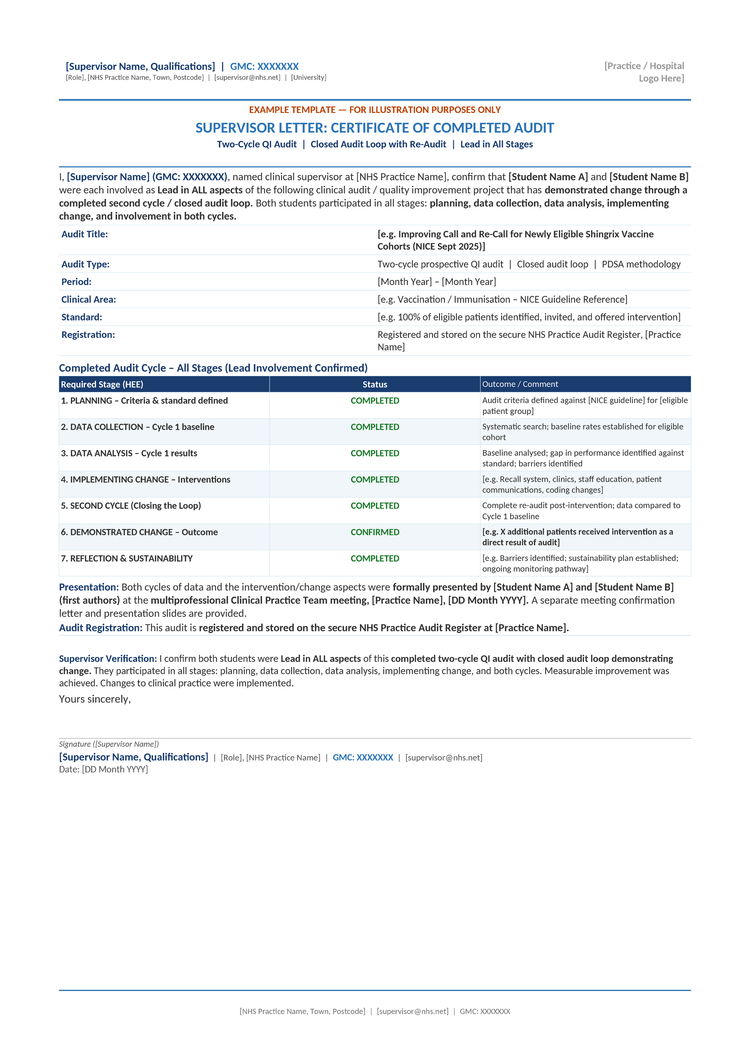
Supervisor Letter: Certificate of Completed Audit
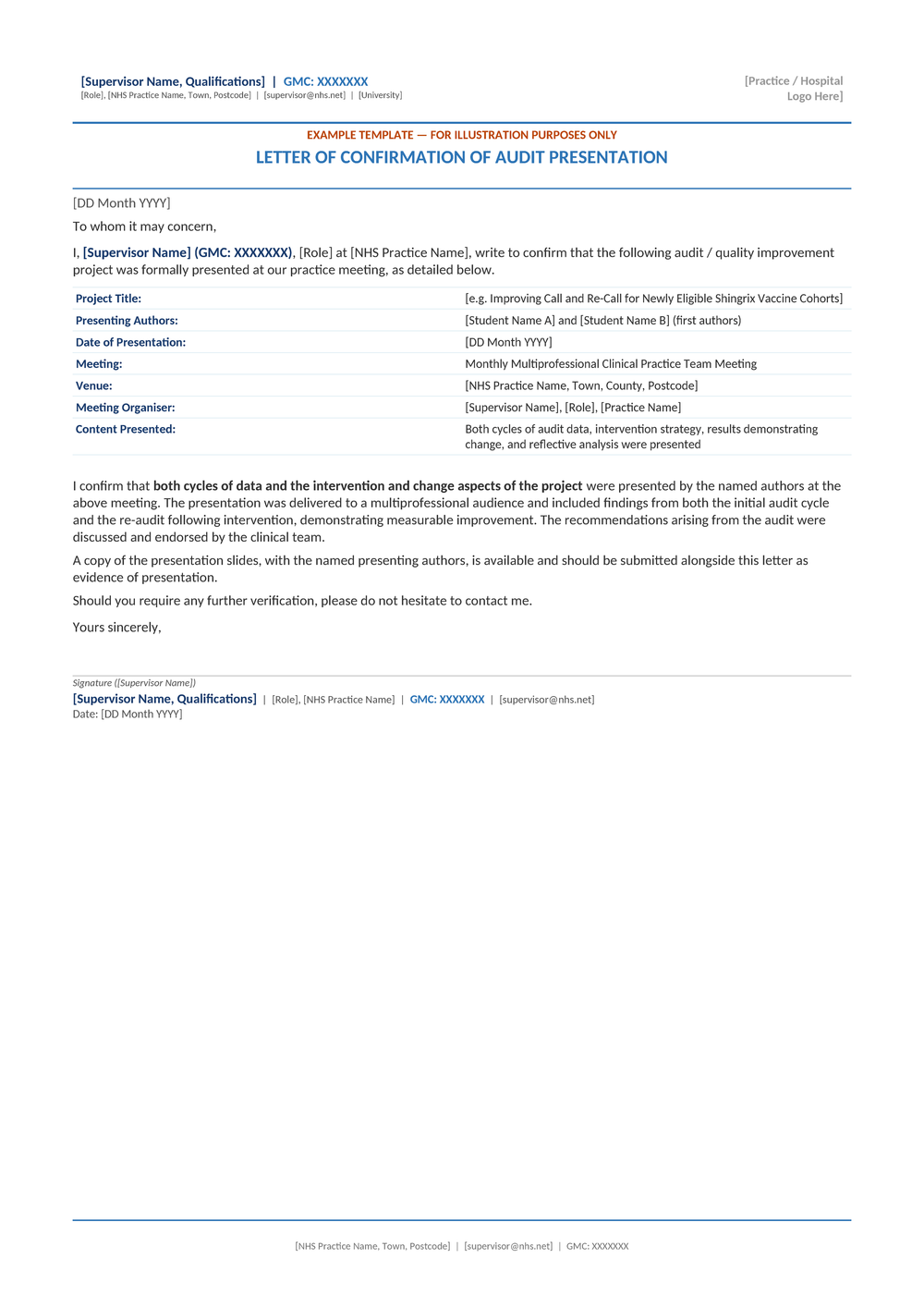
Letter of Confirmation of Audit Presentation
How to use these templates: Ask your clinical supervisor to produce certificates in a similar format. The critical elements are the use of exact HEE terminology ("Lead in ALL aspects," "demonstrated change through a completed second cycle / closed audit loop"), the supervisor's GMC number, and a physical or digital signature. The tabulated audit cycle stages provide clear evidence for Qpercom reviewers.
Research, Publications & Presentations
How academic output is scored and how to maximise your evidence from medical school onwards.
Publications Scoring Hierarchy
Research publications are scored in most specialty training applications. For IMT, first authorship on PubMed-cited papers achieves maximum points. For CST, publications require a PubMed ID or DOI/ISBN for verification. Even case reports and journal letters score points — they are an accessible starting point for medical students.
| Publication Type | Score Level | Accessibility for Students |
|---|---|---|
| First author, PubMed-indexed original research | ⭐ Maximum | Difficult — requires significant research involvement |
| Co-author, PubMed-indexed research paper | ⭐ High | Moderate — join an existing research team |
| First author, case report or case series | ⭐ Mid–High | Very accessible — ask consultants about interesting cases |
| Letter to editor, journal correspondence | Low–Mid | Highly accessible — respond to published articles |
| Conference abstract (published in proceedings) | Low–Mid | Accessible — submit audit/QI findings to regional meetings |
| Audit published in peer-reviewed journal | ⭐ Mid–High | Moderate — follow SQUIRE guidelines |
The BMJ has published guidance on how to publish audit (BMJ 2007;334:gp26), noting that while approximately 1,200 audit-related articles appear in EMBASE over an 18-month period, only a fraction reach core clinical journals.
Presentations Scoring Hierarchy
| Presentation Level | Scoring Impact | Accessibility |
|---|---|---|
| Oral presentation at international peer-reviewed conference | ⭐ Maximum | Competitive — requires accepted abstract |
| Oral presentation at national peer-reviewed conference | ⭐ High | Moderate — specialty conferences, RCS Audit Symposium |
| Poster presentation at national/international conference | Mid | Accessible — many conferences welcome junior doctor posters |
| Oral presentation at regional/local meeting | Low–Mid | Highly accessible — hospital grand rounds, practice meetings |
Important for CST applicants: Only personally delivered presentations count. Presentations requiring payment without genuine peer review are invalid. Ensure you obtain a meeting confirmation letter from the organiser as evidence.
Teaching Experience & Training in Teaching
Teaching is scored in most specialty applications and is one of the most accessible domains for medical students.
Teaching is typically divided into two sub-domains: teaching experience (delivering sessions) and training in teaching (formal qualifications). Developing and delivering your own teaching programme scores significantly higher than individual sessions.
Organise a Teaching Series
Design and deliver a structured programme of 4+ sessions for medical students or junior peers. This scores for both "teaching experience" and "leadership." Obtain a consultant letter confirming your role with their name, GMC number, and dates.
Collect Formal Feedback
Use structured feedback forms for every session. Demonstrating that you reviewed feedback and adapted your teaching shows reflective practice. Keep copies of all feedback forms as evidence for Qpercom upload.
Gain a Teaching Qualification
For IMT, minimum 6 hours of training in teaching is required. For CST, a formal teaching course provides evidence. A PGCert in Medical Education or equivalent scores maximum points in several specialties including Clinical Radiology.
Specialty-Specific Scoring Details
Expand each specialty below for detailed scoring guidance.
Internal Medicine Training (IMT) 2026
IMT uses a self-assessment scoring system at shortlisting with a maximum of 30 points across 6 domains, plus a 5-point bonus for applicants who only apply to the joint IMT/ACCS-IM vacancy in Round 1. The six domains are: postgraduate degrees (excluding MRCP), training in teaching (minimum 6 hours), quality improvement/audit (PDSA or recognised QI methodology), presentations, publications (PubMed first authorship = maximum), and MRCP(UK) exam progress. There is no portfolio station at interview — self-assessment is used for shortlisting. Randomised audits may verify claims.
Core Surgical Training (CST) 2026
CST uses a portfolio station at interview contributing 45% of the total score. Five domains are assessed using letter grades A–E: quality improvement/audit, publications, presentations, teaching, and commitment to surgery. Assessors spend ~10 minutes reviewing uploaded evidence, then discuss two achievements for ~15 minutes. An index sheet is mandatory — missing it scores zero. Evidence must include consultant letters with name, GMC number, and dates for each item.
Clinical Radiology ST1 2026
For 2026, Radiology has five portfolio domains: Commitment to Radiology (double-weighted), Leadership & Management, Teaching & Training, Academic Achievements (including audit, publications, presentations with imaging focus), and one additional domain. Portfolio contributes 40% of total, interview 60%. At least one taster week in radiology is essential. Achievements must be within 10 years of the application deadline.
Ophthalmology ST1 2026
Ophthalmology uses a self-assessment portfolio with max 47 points across 8 domains covering clinical experience, research, prizes, and commitment. MSRA and portfolio are equally weighted. A minimum 40% portfolio score is required for interview, and final selection is 50% interview + 50% portfolio evidence.
Paediatrics (RCPCH) ST1 2026
Paediatrics uses application form scoring with 30 points per assessor across four domains: Transferable Clinical Capabilities, Academic Achievements, Clinical Experience & Reflection, and Audit/Quality Improvement Projects. Evidence is provided as written examples directly on the Oriel form.
GP Training (GPST) 2026
GP training allocation is determined entirely by MSRA performance. There is no portfolio scoring, no interview, and no selection centre. Audit, QI, research, publications, and teaching are not scored. However, building a portfolio remains valuable for long-term career development, appraisals, and potential future applications to other specialties or academic posts.
Strategic Timeline: When to Start Building Evidence
A practical action plan from medical school through to specialty application.
Years 3–4: Foundation Building
Begin your first clinical audit during a GP or hospital placement. Choose a topic with clear NICE guideline standards. Start contributing to research projects for co-authorship opportunities. Deliver peer teaching sessions and collect feedback forms. Apply for medical student prizes.
Year 5: Evidence Consolidation
Complete your first closed-loop (two-cycle) audit during a clinical attachment. Present findings at a practice/departmental meeting and obtain a supervisor certificate and meeting confirmation letter. Submit a case report or audit abstract for publication. Organise a teaching series for younger students. If targeting surgery, begin taster weeks.
FY1: Strategic Portfolio Development
Complete your second closed-loop audit. Submit abstracts to national conferences. Write up your audit for journal publication following SQUIRE guidelines. Develop a formal teaching programme — this scores for both "teaching" and "leadership." Pursue training-in-teaching courses (minimum 6 hours for IMT). Take Part 1 specialty exams if applicable.
FY2: Application Readiness
Ensure all evidence documents are properly formatted, signed, and ready for Qpercom upload. Verify supervisor letters use exact HEE terminology. Check publications have PubMed IDs or DOIs. Complete self-assessment scoring on Oriel carefully — all achievements must be completed at the time of application. You cannot score for work in progress.
Guidance for International Medical Graduates (IMGs)
Specific considerations for IMGs building portfolio evidence for UK specialty training applications.
International Medical Graduates face the same portfolio requirements as UK-trained doctors when applying through Oriel. In the context of the 2026 prioritisation changes, a strong, well-documented portfolio is even more critical for competitive differentiation.
Documentation Standards
All evidence must meet UK formatting standards. Supervisor letters must include a GMC number (or equivalent registration). Non-English documents must be professionally translated. Audit reports should use UK terminology and reference UK guidelines (NICE, SIGN).
UK Clinical Experience
Completing audits in UK NHS settings carries significant weight. Consider clinical attachments or observer posts that provide opportunities for supervised audit completion with a named GMC-registered supervisor who can provide properly formatted certificates.
Portfolio Pathway (CESR)
For experienced IMGs seeking consultant registration, the Portfolio Pathway (formerly CESR) requires extensive evidence including workplace-based assessments, multi-source feedback, audit evidence, teaching records, and multi-consultant references.
The BMJ Careers guide for IMG specialty training applications provides an excellent overview of the full process, including uncoupled versus run-through specialties, the IMT application structure, and GP training via the International Induction Programme.
Official Resources & Further Reading
Start Building Your Portfolio Today
MD ACUMEN provides supervised clinical placement opportunities at NHS GP practices where medical students can complete two-cycle audits, present at multiprofessional meetings, and receive properly formatted HEE-compliant certificates for their portfolio evidence packages.
Legal & Disclaimer · enquiry@mdacumen.com